Լուսինե Վարդանյան1,2, Սամսոն Խաչատրյան2
1Ինֆեկցիոն հիվանդությունների ազգային կենտրոն (ԻՀԱԿ-Նորք), Երևան, Հայաստան
2Նյարդաբանության և նեյրովիրաբուժության ամբիոն, ՀՀ ԱՆ Ակադ. Ս.Խ. Ավդալբեկյանի անվան առողջապահության ազգային ինստիտուտ, Երևան, Հայաստան
ԱՄՓՈՓԱԳԻՐ
Ներածություն. Նոր կորոնավիրուսային վարակը (COVID-19) հիմնականում ախտահարում է շնչառական համակարգը։ Բայց կան բավականին շատ տեղեկություններ նյարդային համակարգի ներգրավվածության և տարբեր նյարդաբանական դրսևորումների մասին: Վարակի ախտորոշման ոսկե ստանդարտ համարվում է հետադարձ տրանսկրիպտազային պոլիմերազային շղթայական ռեակցիան (ՀՏ-ՊՇՌ) սուր նոր կորոնավիրուսային վարակի համար (SARS-CoV-2): Բայց կան կուտակվող տվյալներ թոքերի բնորոշ ախտահարման և ՀՏ-ՊՇՌ բացասական արդյունքների մասին SARS-CoV-2-ի դեպքում:
Դեպքերի նկարագրություն. Նկարագրվում է երկու կլինիկական դեպք (երկու տղամարդ՝ 64 և 69 տարեկան), երբ ըստ կլինիկական, ճառագայթաբանական և համաճարակաբանական տվյալների առկա է եղել COVID-19, որի ֆոնին զարգացել է գեներալիզացված միոկլոնուս, ընդ որում մեկի մոտ հետագայում՝ նաև ցնցումային էպիլեպտիկ ստատուս: Հիվանդների տվյալները վերցվել են Ինֆեկցիոն հիվանդությունների ազգային կենտրոնի բժշկական փաստաթղթերից։ Այս ուսումնասիրությունը հաստատվել է «Նորք» ինֆեկցիոն կլինիկական հիվանդանոցի ներքին վերանայման խորհրդի կողմից։ Պացիենտի նույնականացման տվյալները պաշտպանելու համար գրառումները անանունացվել են: Երկու հիվանդն էլ հոսպիտալացվել են ռենտգենաբանորեն հաստատված երկկողմանի բազմասեգմենտային ինտերստիցիալ թոքաբորբով (COVID-19-ին բնորոշ) և գեներալիզացված միոկլոնուսով: Երկուսն էլ SARS-CoV-2 RT-PCR-ի բացասական արդյունքներ են ունեցել: Գեներալիզացված միոկլոնուսը եղել է ինչպես դրական, այնպես էլ բացասական բաղադրիչներով: Երկուսն էլ հերքել են ալկոհոլի կանոնավոր օգտագործման անամնեզը և հոսպիտալացման պահի դրությամբ նյութափոխանակային լուրջ խնդիրներ չեն ունեցել:
Եզրակացություն. Հայտնի է, որ COVID-19 վարակը կարող է ազդել նյարդային համակարգի գրեթե բոլոր հատվածների վրա և դրսևորվել տարատեսակ նյարդաբանական համախտանիշներով։ Ներկայացված դեպքերը, որոնք առաջին անգամ են հաղորդվել մեր հիվանդանոցից, հուշում են, որ միոկլոնուսի առաջացումը COVID-19 համաճարակի ժամանակ թերևս հազվադեպ երևույթ չէ։ Լրացուցիչ ուսումնասիրություններ են պահանջվում կենտրոնական նյարդային համակարգի վնասման մեխանիզմները և միոկլոնուսի առաջացման համար պատասխանատու հատվածները հայտնաբերելու, ինչպես նաև՝ բուժման օպտիմալ սխեմա մշակելու համար: Նաև դեռևս քննարկման առարկա է՝ արդյոք կապ կա կրծքավանդակի համակարգչային շերտագրության բնորոշ օջախների և քիթ-ըմպանային թեստի բացասական արդյունքների միջև:
Հիմնաբառեր. COVID-19, նյարդաբանական բարդություններ, գեներալիզացված միոկլոնուս, ՊՇՌ-բացասական:
DOI:10.54235/27382737-2022.v2.1-58
INTRODUCTION
The respiratory system is the principal target of coronavirus disease 19 (COVID-19), which is diagnosed mainly by reverse transcriptase polymerase chain reaction (RT-PCR) for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) [1,2]. However, there is increasing evidence of typical lung involvement and negative RT-PCR results for SARS-CoV-2 [3].
COVID-19 infection is also associated with a wide spectrum of neurological syndromes affecting the entire neuraxis. Early recognition and management of COVID-19-related neurological disorders is challenging. Myoclonus has been reported to occur in other viral infections as well [4], but data on association with SARS-CoV-2 remain scarce. Some case reports and case series have started to emerge on this topic [5,6]. They speculate on the possible causes and levels of myoclonus generation.
Our aim was to report two cases of generalized myoclonus in patients with bilateral polysegmental interstitial pneumonia due to RT-PCR-negative COVID-19.
The data were obtained from medical records of the National Center of Infectious Diseases (NCID), Yerevan, Armenia. This report was approved by the Institutional Review Board of the “Nork” Infectious Diseases Clinical Hospital, Yerevan, Armenia. Records were anonymized to protect patients’ personal information.
CASE REPORTS
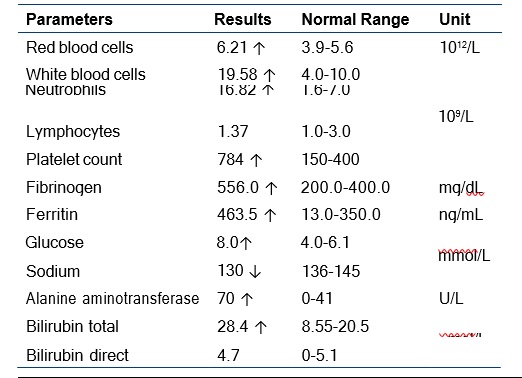
Patient 1. A 64-year-old man was admitted to the emergency department (ED) of NCID because of 20-day history of fever. One week after fever onset, he developed bilateral irregular jerky movements. Neurological status showed no meningeal and focal signs. But there was generalized spontaneous and stimulus-sensitive myoclonus present, with both positive and negative components in upper and lower extremities bilaterally, also involving facial and pharyngeal regions. The patient denied any chronic illnesses or alcohol abuse. The patient was diagnosed with COVID-19 pneumonia based on the clinical and radiological picture. The chest X-ray revealed bilateral interstitial polysegmental pneumonia, with an affected lung surface of 50%. His nasopharyngeal swab for SARS-CoV-2 RNA was negative. Routine blood tests included a complete blood count, coagulation profile, and serum biochemical tests (including renal and liver function, glucose, and electrolytes). Briefly, the plasma samples of the patient were analyzed with a chemiluminescent immunoassay (CLIA) based on the ACCENT 200 Clinical Biochemistry Analyser: deviations from normal values are shown in Table 1.
Table 1. Abnormal laboratory test results: Patient 1
The preliminary diagnosis was of COVID-19-related generalized myoclonus. Brain magnetic resonance imaging (MRI) and electroencephalography (EEG) were planned. Levetiracetam was prescribed as a symptomatic treatment, as it is used as a first-line treatment for myoclonus [7]. However, the patient refused hospital treatment and further investigations and was discharged home the next day.
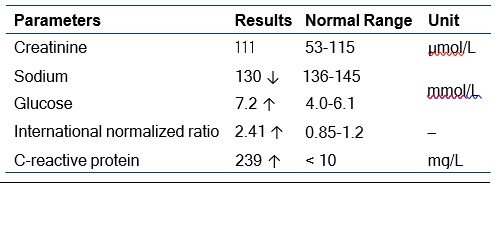
Patient 2. A 69-year-old male patient was admitted to the ED with a 15-day history of fever, malaise, and fatigue. He was treated with moxifloxacin, ceftriaxone, but fever persisted, so he was admitted to the NCID. Three days before admission, jerky movements appeared in both upper and lower extremities. He had a medical history of type 2 diabetes mellitus, arterial hypertension, and thyroidectomy. He was taking antihypertensives, metformin 1000 mg/day, and L-thyroxine 150 μg/day. He was diagnosed with COVID-19 pneumonia based on a chest X-ray that revealed bilateral interstitial polysegmental pneumonia with 90% lung surface involvement. The epidemiological history suggested contact with a SARS-CoV-2-positive patient. His nasopharyngeal swab for SARS-CoV-2 RNA was, however, negative. Complete blood count was normal. Some other laboratory test results are shown in Table 2.
The neurological examination revealed no meningeal and focal signs. However, irregular bilateral myoclonic jerks, predominantly in the upper extremities were present. A preliminary diagnosis of generalized myoclonus was made. Brain MRI and EEG were planned together with a check of thyroid-stimulating hormone (TSH) and free thyroxine (T4-free) levels. Levetiracetam was prescribed as a symptomatic treatment, but hours later the patient developed repetitive generalized tonic-clonic seizures (GTCS) and was transferred to the Intensive Care Unit (ICU). In the ICU, despite the initiated treatment with anticonvulsive medications (carbamazepine and diazepam), GTCSs persisted (convulsive status epilepticus), and it was decided to transfer him to a multidisciplinary hospital to continue treatment.
Table 2. Laboratory tests: Patient 2
DISCUSSION
There is emerging evidence of various neurological associations and complications in COVID-19 patients. There are many theories about potential neurotropic mechanisms of SARS-CoV-2. There are two main possible routes for virus entry to the central nervous system (CNS): hematogenous and neuronal retrograde transmission [8]. So myoclonus can be secondary to brain damage, taking into account the possible ability of SARS-CoV-2 for transneuronal spread via the olfactory bulb [9]. Also it is thought that myoclonus in COVID-19 may be an immune-mediated disorder [5].
The main limitation of each of these two cases is that SARS-CoV-2 PCR-assay was negative. However, we have done the test only once, they came to our side 15-20 days after fever onset, and they were discharged soon (one by will, and second – because of gradual worsening of his condition). The diagnostic accuracy of many of the available RT-PCR tests for detecting SARS-CoV-2 may be lower, than optimal. False-negative PCR result is also a possibility [10,11].
We would like to mention that no other potential causes for the myoclonus were identified in these patients. Both patients denied a history of regular alcohol consumption and had no major metabolic problems at the time of admission. We also have not done brain MRI, EEG, or electromyography. The reason for this was that the NCID is not multidisciplinary and does not possess the specified diagnostic equipment. It is also impossible to ignore the circumstances in hospitals during the peak of the pandemic and the war (Armenian-Azerbaijani war, from 27 September 2020 till 10 November 2020) at the same time.
CONCLUSION
It is well known that COVID-19 infection can affect virtually the entire neuraxis and manifest with various neurological syndromes. The presented cases, firstly reported in our hospital, suggest that the occurrence of myoclonus with possible COVID-19 might not be uncommon. Further research is essential to determine the underlying mechanisms of neurological syndromes in patients with SARS-CoV-2 infection to guide the treatment. In addition, whether there is an association between typical chest CT findings and negative naso-pharyngeal smears is still a matter of debate.
ACKNOWLEDGEMENTS
This study was made possible by the hard work and dedication of multiple investigators. The authors thank all of the volunteers for participating in this study and study personnel for their assistance in enrollment and follow-up visits. Special gratitude to the leadership of the NCID and Dr. Lyudmila Niazyan, Principal Investigator of the “Clinical and Epidemiological Features of COVID-19 in Armenia” research project, for technical assistance.
REFERENCES
- Goudouris ES. Laboratory diagnosis of COVID-19. J Pediatr (Rio J). 2021;97(1):7-12
- Dramé M, Tabue Teguo M, Proye M et al. Should RTPCR be considered a gold standard in the diagnosis of COVID-19? J Medical Virol. 2020;92(11):2312-2313
- Chen Z, Li Y, Wang X et al. Chest CT of COVID-19 in patients with a negative first RT-PCR test Comparison with patients with a positive first RT-PCR test. Medicine (Baltimore). 2020;99(26):e20837
- Delucchi V, Pavlidis E, Piccolo B, Pisani F. Febrile and postinfectious myoclonus: case reports and review of the literature. Neuropediatrics. 2015;46(1):26-32
- Rábano-Suárez P, Bermejo-Guerrero L, MéndezGuerrero A et al. Generalized myoclonus in COVID-19. Neurology. 2020;95(6):e767-e772
- Foucard C, San-Galli A, Tarrano C et al. Acute cerebellar ataxia and myoclonus with or without opsoclonus: a parainfectious syndrome associated with COVID-19. Eur J Neurol. 2021;28(10):3533-3536
- Caviness JN. Treatment of myoclonus. Neurotherapeutics. 2014;11(1):188-200
- Desforges M, Le Coupanec A, Dubeau P et al. Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses. 2019;12(1):14
- Desai I, Manchanda R, Kumar N et al. Neurological manifestations of coronavirus disease 2019: exploring past to understand present. Neurol Sci. 2021;42(3):773-785
- Brogna B, Bignardi E, Brogna C et al. Typical CT findings of COVID-19 pneumonia in patients presenting with repetitive negative RT-PCR. Radiography (Lond). 2021;27(2):743-747
- Quaia E, Baratella E, Crimi F et al. High-resolution CT features in patients with COVID-19 pneumonia and negative nasopharyngeal and oropharyngeal swabs. Pulmonology. 2021;27(4):351-353